
The 2019 Novel Coronavirus was identified as the cause of an outbreak of respiratory illness, referred to as COVID-19. It was first detected in Wuhan, China on Dec. 12, 2019. Because this disease already has begun to spread worldwide, it is important that water sector professionals keep informed on the attributions of this virus and any measures needed to protect both workers and public health, in general.
Disclaimer: The information posted here is a summary of current knowledge about this emerging viral pathogen. The state of knowledge will evolve as additional investigation and research is conducted, so continuous review of reputable sources and websites is advised.
Extent of the 2019 Novel Coronavirus Outbreak
This virus is a member of the Coronavirus family. On Feb. 5, 2020, the World Health Organization reported 24,554 cases and 492 deaths in 25 countries worldwide, with the vast majority (24,363 cases and 491 deaths) in China. As of February 17, 2020, this number has globally increased to 71,429 confirmed cases, 70,635 of which are located in China. This large increase in case numbers is mainly due to a change in reporting by the WHO.
The U.S. reported its first confirmed case of person-to-person spread with this virus on Jan. 30, 2020. As of Feb. 16, 2020, there were 15 confirmed cases in the US. The most up-to-date CDC data are available online.
In Canada, eight cases of COVID-19 have been confirmed as of Feb. 16, 2020. Canadian case numbers are being updated daily by the Public Health Agency of Canada.
Based on the sharp increase in number of COVID-19 infections, on Jan. 30, 2020, the World Health Organization (WHO) declared the current outbreak to be a public health emergency of international concern.
Have we seen this virus before? What do we know about its origin?
The virus, technically named SARS-CoV-2, is a newly identified virus, but it is the seventh Coronavirus known to infect humans. The resutling illness is referred to as COVID-19. This virus is in the same Coronavirus family as severe acute respiratory syndrome Coronavirus (SARS-CoV or SARS) and Middle East respiratory syndrome Coronavirus (MERS-CoV or MERS), which caused the two previous Coronavirus outbreaks in 2003 (SARS) and 2012 (MERS).
Since SARS and MERS are from the same family of coronaviruses, they have similar physical and biochemical properties and comparable transmission routes as COVID-19. In the absence of COVID-19 specific data, we rely on SARS, MERS, and coronavirus surrogate data to extrapolate, assess, and manage risk. See a comparison with these viruses.
In addition to the seven coronaviruses known to infect humans, many other coronaviruses are known to infect animals. Viruses that infect animals do not normally infect humans and vice versa, but mutations in the viral genetic material can occur naturally and lead to animal-to-person spread, formally known as zoonotic transmission.
Initially, many of the patients in the outbreak in Wuhan reportedly had some link to a large seafood and animal market suggesting animal-to-person spread. Later on, an increasing number of patients with COVID-19 had no exposure to animals, indicating person-to-person transmission is occurring.
This has occurred with other Coronaviruses such as SARS and MERS, which originated from animal reservoirs, spread into the human population, and then continued to spread by person-to-person contact. A recent publication links COVID-19 to bats. The CDC posts updated information on this topic.
How is COVID-19 transmitted, and how contagious is it?
While many questions remain regarding transmission of COVID-19, most often Coronaviruses spread from person-to-person during close contact — about 2 m (6 ft). Person-to-person spread is thought to mainly occur via respiratory droplets produced when an infected person coughs or sneezes, similar to how influenza and other respiratory pathogens spread. These droplets can land in the mouths or noses of people who are nearby or possibly be inhaled into the lungs. Close contact generally does not include brief interactions, such as walking past a person.
With most respiratory viruses, people are thought to be most contagious when they show symptoms of infection. However, some viruses can be contagious prior to symptoms development, and the COVID-19 has been reported to have spread from an asymptomatic infected patient to a close contact.
The rate at which a person can get COVID-19 by touching a contaminated surface or object (i.e., fomites) and then touching their own mouth, nose, or possibly their eyes is unclear. We also do not know if viral particles can be aerosolized from water or suspended into air after settling and remain infective. While such routes can occur for other coronaviruses, the European Centre for Disease Prevention and Control states that there is currently no evidence to support airborne transmission of the novel Coronavirus. A precautionary approach should be taken until studies eliminate other routes of transmission. Epidemiological studies also suggest that transmission rates of COVID-19 currently might be higher than those of SARS and MERS. Scientists have estimated that each person with the new Coronavirus could infect somewhere between 1.5 and 3.5 people without effective containment measures, according to “Early Transmissibility Assessment of a Novel Coronavirus in Wuhan, China,” in the Elsevier SSRN (Social Science Research Network).
Is COVID-19 present in wastewater?
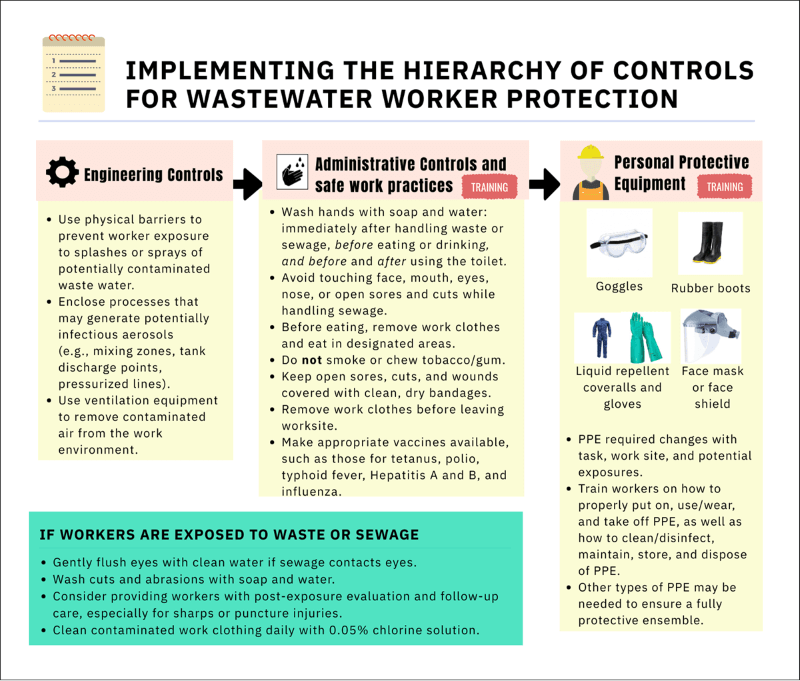
Recent information suggests that COVID-19 may be transmitted through the fecal-oral route. The virus RNA was detected in patient stool after scientists noticed that some patients infected with the COVID-19 virus experienced diarrhea in the early stages of infection instead of a fever, the latter being more common. A recent paper, “First Case of 2019 Novel Coronavirus in the United States,” in the New England Journal of Medicine also confirmed the virus RNA detection in feces. OSHA recommends that workers handle solid waste contaminated with COVID-19 as they would other regulated Category B medical waste, corresponding with the recommendations of other organizations. If the recovery of infectious particles from feces or wastewater at potentially infective doses is confirmed at a future date, this recommendation may have to be revised.
Detection of viruses by molecular techniques provides no indication that the virus is infectious. It remains to be seen if infectious virus particles are excreted in patients' feces and urine, and if so, how well the viruses are able to survive in wastewater.
Previous studies investigating persistence of coronavirus surrogates and SARS in wastewater highlight that in the absence of disinfection, the virus can survive in wastewater from hours to days. In 2003, research on SARS had suggested that sewage was implicated in the infection of a cluster of cases in the Amoy Gardens apartment block in Hong Kong. A recent report indicated possible COVID-19 transmission through sewage pipes in a building in Hong Kong, but this remains to be confirmed.
However, previous work also highlights that SARS can readily be disinfected when chlorine dosing produces a free chlorine residual between 0.2 and 0.5 mg/L for municipal wastewater. While Ebola virus is different, it is reassuring that the article, “Persistence of Ebola Virus in Sterilized Wastewater,” similarly showed that no virus was recovered at doses of 5 and 10 mg/L of chlorine and a 3.5 log reduction was achieved in the presence of free chlorine residual of 0.16 mg/L for 20 seconds. These results imply that standard municipal wastewater system disinfection and hyper (or shock) chlorination practices may be sufficient to control the virus provided utilities monitor free available chlorine during treatment to ensure it has not been depleted.
Wastewater Treatment and COVID-19
Disinfection systems at water resource recovery facilities (WRRFs) and the associated regulatory requirements were developed to be protective of a broad spectrum of potential pathogens. The recent coronavirus serves as another example of the importance of this infrastructure for protecting public health.
On Feb. 5, 2020, the U.S. Occupational Safety and Health Administration (OSHA) released its new wastewater worker guidance stating that current disinfection conditions in WRRFs, such as oxidation with hypochlorite or peracetic acid, and inactivation by ultraviolet irradiation, are expected to be sufficient to protect wastewater workers and public health. The recommendation is based on coronavirus disinfection data from healthcare settings and corresponds with OSHA’s position on the susceptibility of coronaviruses to disinfection.
These recommendations are likely to be broadly applicable, although more research may be warranted for disinfectants such as peracetic acid and combined chlorine (chloramines), where coronavirus specific data is lacking or evidence suggests higher bacterial susceptibility to disinfection compared to viruses. Although coronaviruses have not been tested, peracetic acid has been found to have some efficacy against some non-enveloped viruses (e.g., Norovirus) that are known to be more resistant than enveloped viruses.
Chlorine is extensively used for wastewater disinfection due to its effectiveness, low cost, and ease of application. It typically reacts with ammonia present in wastewater to form combined chlorine (chloramines), which behaves differently than free chlorine during disinfection. Thus, it is important for each facility to understand the chlorine species that are present and their relative abundance within the disinfection process. Additional research could provide reassurance on the effectiveness of wastewater disinfection processes, specifically against coronaviruses and at lower doses and contact times.
•••
How Can I Stay Informed?
The organizations below are reputable and reliable sources that are frequently updated.
In an effort to increase transparency and communication, major publishers have created Coronavirus information centers, where relevant and current research is freely available. This includes Springer Nature, Elsevier and Wiley. Several major journals have done the same, including: The Lancet, New England Journal of Medicine and The British Medical Journal.